About: Poor Health


Hospitals and family doctors, the mainstays of health care, are pulling out of poor city neighborhoods, where the sickest populations live.
A Pittsburgh Post-Gazette/Milwaukee Journal Sentinel analysis of data from the largest U.S. metropolitan areas shows that people in poor neighborhoods are less healthy than their more affluent neighbors but more likely to live in areas with physician shortages and closed hospitals.
At a time when research shows that being poor is highly correlated with poor health, hospitals and doctors are following privately insured patients to more affluent areas rather than remaining anchored in communities with the greatest health care needs.
The Post-Gazette/Journal Sentinel analysis shows that nearly two-thirds of the roughly 230 hospitals opened since 2000 are in wealthier, mostly suburban areas.
As health systems open those facilities, they have been closing their urban counterparts. The number of hospitals in 52 major cities in the United States has fallen from its peak of 781 in 1970 to 426 in 2010, a drop of 46 percent.
Most of the facilities closed were small to mid-size community hospitals in poor urban neighborhoods and public hospitals, leaving many low-income neighborhoods with no safety-net hospital.
New York City's boroughs have lost more than 20 hospitals since 1990. Detroit has gone from dozens in the 1960s to four.
Locally, in the distressed community of Braddock, residents fought a long battle against the closure of their community's hospital. UPMC shut down the Braddock facility and razed the building in 2010 as protesters gathered in the street, tolling a bell for the 104-year-old institution.
Since 1988, Milwaukee County has lost its public hospital and five city hospitals.
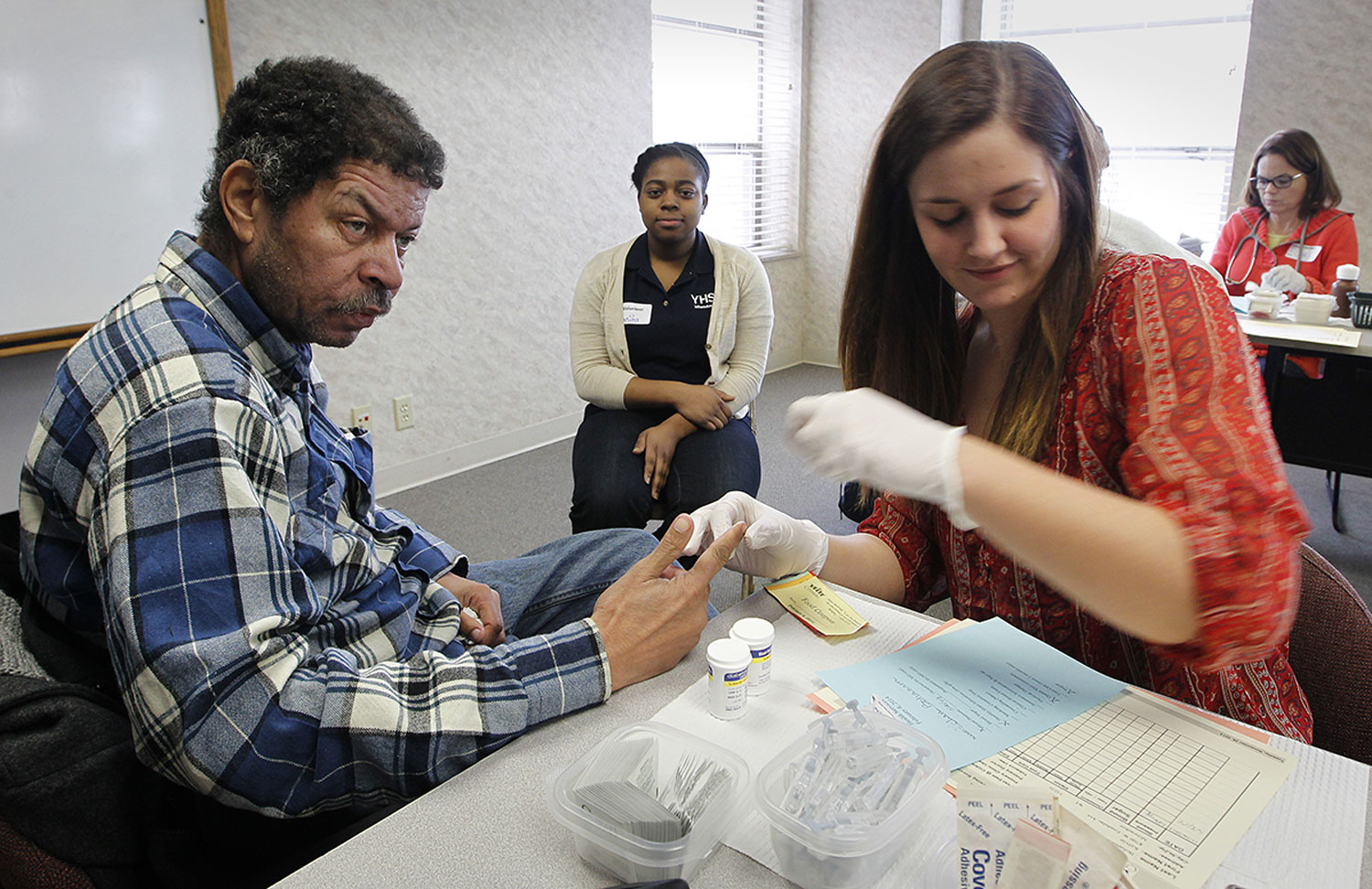
One of those is the former Milwaukee Hospital. A small nonprofit called City on a Hill now operates in a wing of the large complex, which overlooks one of Milwaukee's poorest neighborhoods. Once a month, when the agency hosts a free clinic on a Saturday, a line forms more than an hour early and stretches down the block.
The closures have been going on for decades.
Between 1990 and 2010 alone, 148 nonprofit hospitals closed in the largest American cities, along with 53 for-profit hospitals.
In addition, five public hospitals closed, according to Alan Sager of Boston University, who has tracked and studied hospital closures in the United States. His research shows it's not just poor-performing hospitals being closed; the ones that shut down often are rated as being more efficient than those that remain.
"In a competitive free market, efficient hospitals would be likelier to survive," he wrote in a paper summarizing some of his research results. "That hasn't happened, providing evidence that no such market is present."
When communities lose hospitals, they lose doctors, too.
The newspapers' data analysis shows that doctors are scarcer in poor neighborhoods: Fifty-eight percent of the nation's 5,800 federally designated "primary care shortage areas" fall in census tracts of highest poverty in the 52 major metropolitan areas. In the 52 metro areas, at least one in five people live in a shortage area. Those areas also tend to have higher than average populations of people with disabilities.
These are typically neighborhoods where people are isolated by poverty. They are less likely to have jobs, less likely to have vehicles and access to healthy food, and more likely to face violence in and outside their homes.
As the presence of health care providers in low-income neighborhoods decreases, a growing body of evidence shows that poor people are more likely to be in poor health – indeed, poverty itself can make people sick.
Think of a child with asthma living in a mold-filled apartment, a man with an infected foot living on the streets and sleeping in his dirty, wet shoes, or a person with diabetes without a refrigerator to store insulin.
Mary Mazul, director of population health management and integration at Wheaton Franciscan Healthcare in Milwaukee, described a conversation with a doctor she knows who works with mostly poor patients, who told her: "Mary, I'm a good doctor but my outcomes aren't so good."
"Health care can't fix poverty, homelessness, racism," Ms. Mazul said.
Early death is the simplest measure of compromised health.
A Centers for Disease Control and Prevention study of U.S. counties conducted by University of Wisconsin researchers showed that the overall rate of death before age 75 was 417 deaths per 100,000. In low-income counties, the average was 480; in higher-income counties, the average was 345. The premature death rate was 39 percent higher in the poor counties that have been losing hospitals and doctors.
Disability rates also are higher among low-income residents. The Post-Gazette/Journal Sentinel analysis of U.S. Census data shows that in the lowest-income areas, an average of 12 percent of the population has disabilities. In the highest-income areas, the average is 5 percent.
It is those higher-income areas, where people are healthier and mobile, that are most likely to get new hospitals. At the same time that UPMC was closing its hospital in Braddock, it was constructing a $250 million hospital in Monroeville, where the average household income is more than twice as high.
"To me it's like free-market fire departments," said Robert Connolly of Common Ground, a Milwaukee community organization that started a health care cooperative last year. "Would anyone advocate building one on a corner across from another one to compete for fire business?"
Or closing down a fire station in a neighborhood with a higher rate of fires?
Mapping poor health
How we analyzed the data
To examine the changing landscape of hospitals in large metropolitan areas, the Pittsburgh Post-Gazette and Milwaukee Journal Sentinel used Provider of Service files from the Centers for Medicare and Medicaid Services. The files, one dating from 1991 and another from 2013, provide snapshots in time of the locations and services offered by the hospitals that were registered with CMS at the time.
The analysis focused on short-term acute care centers -- that is, hospitals with emergency rooms -- in metro areas with at least 1 million population.
For measures of poverty, median income and disability, the newspapers used the five-year American Community Survey from the U.S. Census bureau. Zip code tabulation areas were assigned to each hospital based on physical location, then compared to the broader metro area.
The newspapers also examined primary care physician shortage areas using data from the U.S. Health Resources and Services Administration. Geographic areas, as well as populations of people, can be considered to be in a shortage area if there are fewer than 1 primary care physician per 3,500 people. In areas of greater need, that figure is 1 doctor to 3,000 people.
Kevin Crowe of the Milwaukee Journal Sentinel staff completed the data analysis. Allan James Vestal of the Journal Sentinel staff designed and built the interactive map.